Susan Azizmohammadi,
Sima Azizmohammadi ![]()
For correspondence:- Sima Azizmohammadi Email: sam_215pv@yahoo.com Tel:+89121057715
Received: 30 June 2016 Accepted: 9 November 2016 Published: 21 December 2016
Citation: Azizmohammadi S, Azizmohammadi S. Antimicrobial susceptibility pattern of Neisseria gonorrhoeae isolated from fertile and infertile women. Trop J Pharm Res 2016; 15(12):2653-2657 doi: 10.4314/tjpr.v15i12.17
© 2016 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
Purpose: To study the prevalence of Neisseria gonorrhoeae in the high vaginal swab samples of fertile and infertile women who were referred to Infertility and Sterility Hospitals, Tehran, Iran as well as investigate their antibiotic resistance pattern.
Methods: Three hundred and twenty high vaginal swabs were taken from fertile and infertile women. The samples were cultured and those that were N. gonorrhoeae-positive subjected to the disk diffusion susceptibility test.
Results: Prevalence of N. gonorrhoeae in fertile and infertile women were 5.26 and 16.92 %, respectively. All isolates harbored orf1 gene. Patients in the age bracket > 40 years were at high risk. N. gonorrhoeae strains showed high level resistance against ampicillin (87.5 %), ciprofloxacin (75 %), tetracycline (71.87 %) and penicillin (68.75 %).
Conclusion: The possible role of resistant N. gonorrhoeae as pathogens causing female infertility constitutes an important finding of the study. The high levels of bacterial resistance against ampicillin, ciprofloxacin, tetracycline, penicillin and spectinomycin, should be taken into account in developing any new guidelines in the management of the infection.
Introduction
Infertility is one of the major serious concerns confronting medical practitioners. Despite all the advances in medical sciences, the main reasons of infertility especially in women are still unknown. Infertility means that couples have been trying to get pregnant with frequent interaction for at least a year with no achievement [1,2]. It has been estimated that about 72.4 million couples are infertile [3]. Majority of women with infertility problems manifest inflammatory changes of the oviduct or surrounding peritoneum. Most of these alterations result from infections [4].
Neisseria gonorrhoeae (the gonococcus) is a Gram-negative diplococcal bacterium which infects only humans. It causes gonorrhea, sexually transmitted infections (STI), Pelvic Inflammatory Disease (PID), ectopic pregnancy, chronic pelvic pain, infertility, acute urethritis, cervicitis and proctitis or pharyngitis [5]. N. gonorrhoeae infections represent 106 million of the estimated 498 million new cases of curable sexually transmitted infection that occur globally every year [5]. Previous studies have estimated 3.4 million cases of gonorrhea among adults in the European countries [5].
One of the best therapeutic options for treatment of the cases of gonorrhea caused by this bacterium is antibiotic therapy. However, antibiotic-resistant N. gonorrhoeae have evolve and spread rapidly [6]. N. gonorrhoeae resistance is commonly observed with penicillin, tetracycline and fluoroquinolones antibiotics [6]. Resistance has also emerged against cefixime, an oral third generation cephalosporin, in recent years [7,8]. Since 2010, cefixime has not been recommended as first-line drug treatment [7,8] following WHO guidelines, stating that an antibiotic should not be used when more than 5 % of N. gonorrhoeae isolates are resistant [9]. Injectable ceftriaxone, in combination with oral azithromycin, are the recommended first line drug treatment [10]. Data regarding the epidemiology, prevalence of antibiotic resistance profile of N. gonorrhoeae in the cases of female infertility is scarce in Iran. Therefore, the present investigation was carried out to study the prevalence of N. gonorrhoeae in the high vaginal swab samples of fertile and infertile women as well as investigate the antibiotic resistance pattern of bacterial isolates.
Methods
Ethical issues
The aspect of human studies in the present study was approved by the ethical committee of Department of Infertility and Sterility of Educational Hospitals, Iran (approval ref no. 20275 MD), and the Research Adjutancy of Hajar Hospital, Tehran, Iran (approval ref no. 45891 MD). The authors conformed to generally accepted scientific principles [11]. All samples were taken from volunteer women who were referred to Infertility and Sterility Hospitals, Iran. Written consents were obtained from the infertile and fertile women or their husbands.
Sample collection
Samples were collected from June to November 2015; a total of 130 high vaginal swab specimens were taken from infertile women. In a primary view, a woman after a year of regular intercourse without prevention was defined as infertile. Vaginal specimens were collected from the ventral fornix without any contact with urine and external parts of reproductive system using speculum and commercial sterile cotton-tipped swabs. All specimens were collected by an expert midwife. One hundred and ninety vaginal swab specimens were also collected from fertile women with no history of infertility.
Culture-based identification of N. gonorrhoeae
All the samples were inoculated directly onto modified Thayer Martin (Thayer Martin + laked sheep blood and the antibiotic supplement (BBL VCNT inhibitor) including colistin (750 µg), nystatin (1250 units), vancomycin (300 µg) and trimethoprim Lactate (500 µg)) and incubated immediately at 34 to 36 °C in an atmosphere of 5 % CO2 for 72 h. Morphologically suggestive colonies were screened by Gram staining and by their positive responses to the oxidase and catalase tests. Positive colonies were subcultured on chocolate supplement agar (Chocolate Polyvitex/Biomérieux®), and their identification confirmed by fluorescent-antibody staining (Baxter Scientific, McGaw Park, Ill).
DNA extraction and PCR confirmation of positive colonies
Genomic DNA was extracted from the bacterial colonies using the commercial genomic DNA extraction kit (Fermentas, Germany) according to the manufacturer’s instruction. The DNA concentration has been determined by measuring absorbance of the sample at 260 nm using spectrophotometer [12]. Presence of N. gonorrhoeae was confirmed with the PCR-based amplification of orf1 gene. Reaction was performed in a final volume of 50 µL containing 5 µL 10 × buffer + MgCl2, 2 mM dNTP, 2 unit Taq DNA polymerase, 100 ng genomic DNA as a template, and 25 picomole of each primer (5'-CAACTATTCCCGATTGCGA-3’ and 5'- GTTATACAGCTTCGCCTGAA-3') (amplify the 221–480 bp region of orf1 gene). PCR was performed using a thermal cycler (Eppendorf Mastercycler 5330, Eppendorf-Nethel-Hinz GmbH, Hamburg, Germany) under the following conditions: an initial denaturation for 10 min at 94 °C and 40 cycles including 94 °C for 30 s, 52 °C for 30 s and 72 °C for 1 min, and a final extension at 72 °C for 5 min. S. aureus ATCC 19424 was used as a positive control and distilled water was used as a negative control. PCR amplification products (15 μl) were subjected to electrophoresis in a 2 % agarose gel in 1X TBE buffer at 80 V for 30 min, stained with SYBR Green.
Evaluation of antimicrobial susceptibility pattern of N. gonorrhoeae
Pattern of antimicrobial resistance was studied using the simple disk diffusion technique. Antibiotic resistance of the N. gonorrhoeae strains against 9 commonly used antibiotics was determined using the Clinical and Laboratory Standards Institute guidelines [20]. Susceptibility of N. gonorrhoeae isolates were tested against ampicillin (10 µg/disk), azithromycin (15 µg/disk), cefixime (5 µg/disk), ceftriaxone (30 µg/disk), ciprofloxacin (5 µg/disk), chloramphenicol (30 µg/disk), penicillin (10 u/disk), tetracycline (30 µg/disk) and spectinomycin (100 µg/disk) antibiotic agents (Oxoid, UK). The diameter of the zone of inhibition produced by each antibiotic disc was measured and interpreted using the CLSI zone diameter interpretative standards [13]. N. gonorrhoeae ATCC 49226 was used as a standard reference strain for quality control of susceptibility testing.
Statistical analysis
The results were transferred to a Microsoft Excel spreadsheet (Microsoft Corp., Redmond, WA) for analysis. Statistical analysis was performed using SPSS/18.0 software (SPSS Inc, Chicago, IL) for significant relationship between the prevalence of bacteria and their antibiotic resistance pattern. The chi-square test and Fisher’s exact 2-tailed test analysis were performed in this study. Statistical significance was regarded at p < 0.05.
Results
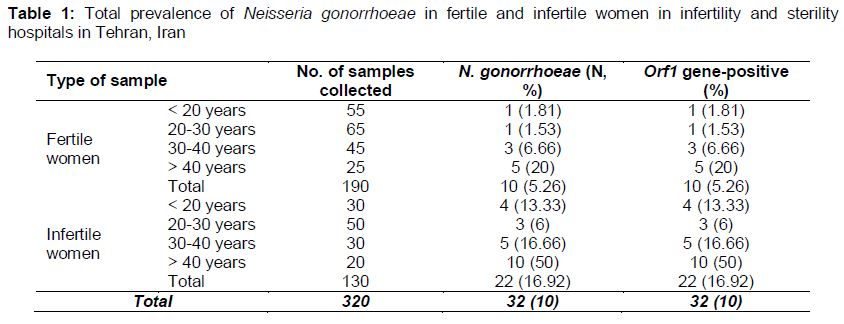
represents the total prevalence of N. gonorrhoeae in fertile and infertile women of Iranian infertility and sterility hospitals. Results showed that 32 out of 320 high vaginal swab samples (10 %) were positive for N. gonorrhoeae. Besides, the prevalence of bacteria in the high vaginal swab samples of fertile and infertile women were 5.26 and 16.92 %, respectively. Those older than 40 years old fertile (20 %) and infertile (50 %) women had the highest prevalence of N. gonorrhoeae. Significant statistical differences were seen for the prevalence of N. gonorrhoeae between fertile and infertile women (p < 0.01). Statistical difference was also seen between the age of women and prevalence of N. gonorrhoeae (p < 0.05). All the N. gonorrhoeae strains were confirmed using the PCR amplification of orf1 gene (). The N. gonorrhoeae isolates were positive for the orf1 gene ().
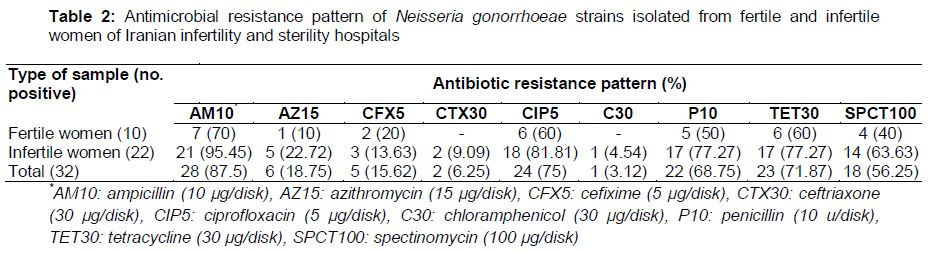
represents the antimicrobial resistance pattern of N. gonorrhoeae strains isolated from fertile and infertile women of Iranian infertility and sterility hospitals. We found that the N. gonorrhoeae strains showed high level resistance against ampicillin (87.5 %), ciprofloxacin (75 %), tetracycline (71.87 %) and penicillin (68.75 %). N. gonorrhoeae isolates of infertile women were more resistant against commonly used antibiotic than those of fertile women (p < 0.05).
Discussion
Infections of the genital tract may be predisposing factors in unexplained infertility. Hormonal disorders that occurred in infertile women can lead to reduced levels of immunity and increase bacterial colonization of vaginal epithelium [14]. Women follicular fluid is not sterile and the levels of cytokines, chemokines and growth factors which are essential for ovarian function [15], secretion of ovarian steroid hormones [15] and development and regression of corpus luteum [16] in follicular fluid of infertile women have been decreased. Therefore, it is not surprising the 16.92 % of high vaginal swab samples of infertile women were infected with resistant strains of N. gonorrhoeae. The present study found high levels of N. gonorrhoeae resistance against ampicillin, ciprofloxacin, tetracycline, penicillin and spectinomycin.
Several investigations have been done in this field all-around the world. Afrasiabi et al [17] reported that gonorrhea was diagnosed in 7 out of 294 (2.38 %) Iranian women which was lower than our results. They showed that the highest levels of resistance was observed for ciprofloxacin (100 %), penicillin G (100 %), ceftriaxone (100 %) and cefepime (100 %), but 28.5 % of isolates showed intermediate sensitivity to tetracycline. Significantly lower prevalence of N. gonorrhoeae were also found among Iranian previously published research [18]. Brunner et al [19] reported that among the 9097 sexually active patients tested, 582 had an N. gonorrhoeae infection (6.39%). The isolates were all sensitive to ceftriaxone and spectinomycin and 581/582 strains were sensitive to cefixime (99.82 %). They also showed a high percentage of detected resistance to penicillin (77 %), tetracycline (86 %), and ciprofloxacin (66 %) which are similar to our findings.
In Iran, as is the case in many other countries, the control of gonococcal infections mostly depended on an effective single-dose antibiotic therapy given at the first clinical presentation of the patient. Prior knowledge of the antimicrobial susceptibility pattern of the particular strain infecting the patient was routinely not established however. With increasing evidence of antimicrobial resistance in gonococcal infections there was a real risk of treatment failure and development of further resistance to antibiotics.
Unfortunately, irregular and indiscriminate prescription of some routine antibiotics including ampicillin, ciprofloxacin, tetracycline, penicillin and spectinomycin in Iranian infertility and sterility hospitals caused high level resistance against them. High prevalence of gonococcal resistance against these antibiotics has been reported previously from United States [20] and United Kingdom [21]. Wit was found that 3.12 % of N. gonorrhoeae strains were resistant against chloramphenicol. Chloramphenicol is only used in the final stages of treatment when other therapeutic agents are not effective, hence a low level of resistance against this antibiotic.
Conclusion
The results of this study highlight the role of N. gonorrhoeae as a possible pathogens of infertility in women, and are a significant contribution to current knowledge on antimicrobial susceptibility of N. gonorrhoeae strains isolated from cases of infertility in Iran. A high level of antimicrobial resistance has been found in the isolated strains. The emergence of resistance against currently recommended antibiotics is worrisome.
Thus, rapid identification of cases of gonococcal female infertility, and also primary treatment with ceftriaxone, cefixime, and azithromycin, and in severe cases with chloramphenicol, may reduce the risk of further complications. Monthly check-up of fertile women and treatment with appropriate antibiotics may reduce the risk of infertility. Changes in the pattern of antibiotic resistance should be taken into account in developing any new treatment guidelines for the infection.
References
Archives


News Updates